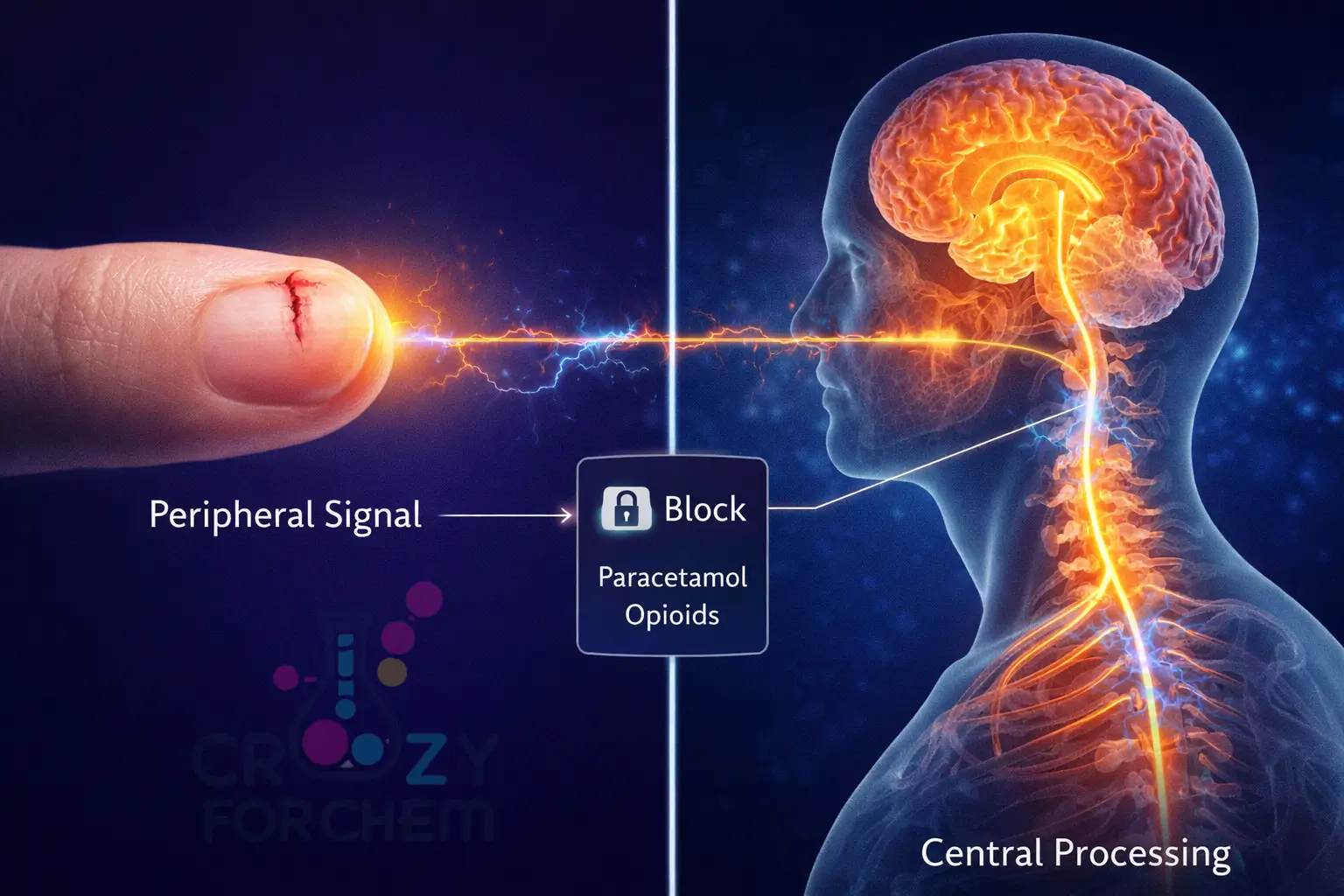
Painkillers don’t ‘find’ pain. After ingestion, they circulate throughout the bloodstream. NSAIDs (like Aspirin) work by blocking COX enzymes everywhere, which stops the production of prostaglandins (pain signals) only where tissue is damaged. Paracetamol acts on the central nervous system to raise your overall pain threshold.
“As a chemist, I don’t see a simple white tablet; I see a precisely engineered molecular delivery system designed to navigate the body’s complex biochemical pathways.”
Walking into a pharmacy, we are met with a vast array of options for relief, yet most consumers rarely stop to wonder about the sophisticated Chemistry of painkillers taking place within their own cells.
Whether it is the throb of a headache or the sharp sting of a cut, pain is a universal human experience, but the science behind how we “switch it off” is a remarkable feat of pharmacology.
A common misconception is that a swallowed pill travels through the body like a heat-seeking missile, heading straight for the source of distress.
In reality, these medications do not “search” for your injury; instead, they circulate throughout your entire body via the bloodstream. To understand how painkillers work, we must first explore the body’s natural alarm system and how these chemical messengers are manipulated to provide relief.
Table of Contents
Understanding the Target: The Body’s Alarm System
Pain is our body’s urgent signal that something is not quite right. It serves a vital protective function, warning us of potential or actual tissue damage.
This complex, multi-faceted experience involves physical, emotional, and psychological factors.
Nociceptors and the Pain Pathway
The experience of pain begins with specialised nerve endings called nociceptors, which are found throughout the skin and tissues.
When you are injured, perhaps by a burn, a cut, or inflammation, these nociceptors detect the harmful stimulus and send electrical impulses along nerve fibres to the spinal cord.
From the spinal cord, the signal ascends to the brain, specifically reaching the thalamus, which acts as a central switching station.
The thalamus routes these signals to the cortex, generating the conscious sensation of pain, including its location and intensity.
Interestingly, certain reflexive responses, such as pulling your hand away from a hot stove, are often processed at the spinal level before the signal even reaches the brain.
Prostaglandins: The Chemical Messengers
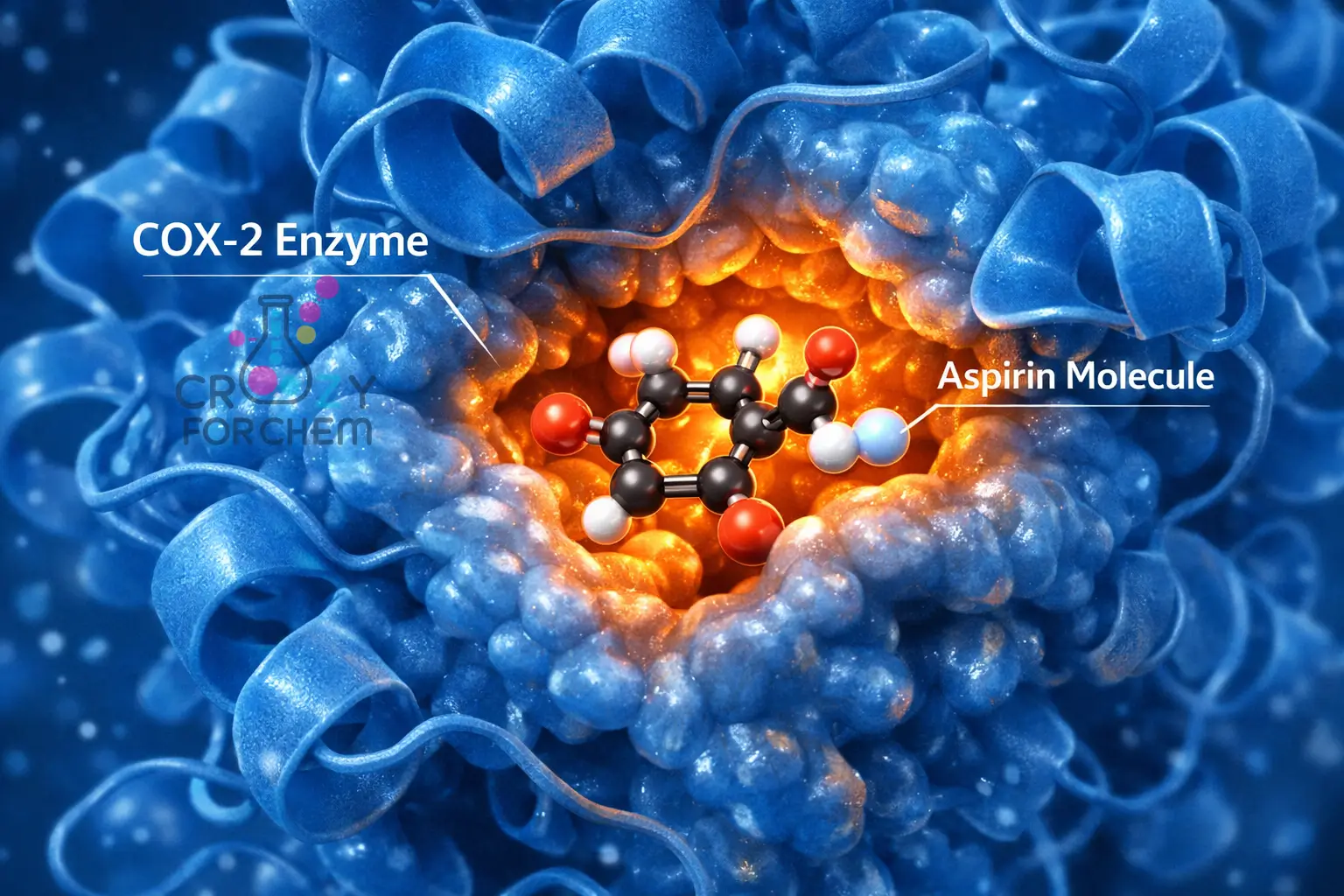
At the molecular level, when cells are damaged or injured, they release a protein (enzyme) called COX-2. This enzyme is responsible for producing chemicals called prostaglandins.
These prostaglandins are key players in triggering pain, swelling, and fever at the site of an injury or infection. They effectively lower the firing threshold of nerves, making them send distress signals to the brain more easily and frequently.
This process is the primary target of the Chemistry of painkillers.
The Big Question: How Do Painkillers Find Pain?
The truth regarding how painkillers find pain is that most of them do not actually “know” where the specific injury is. Instead, they work through a systemic broadcast.
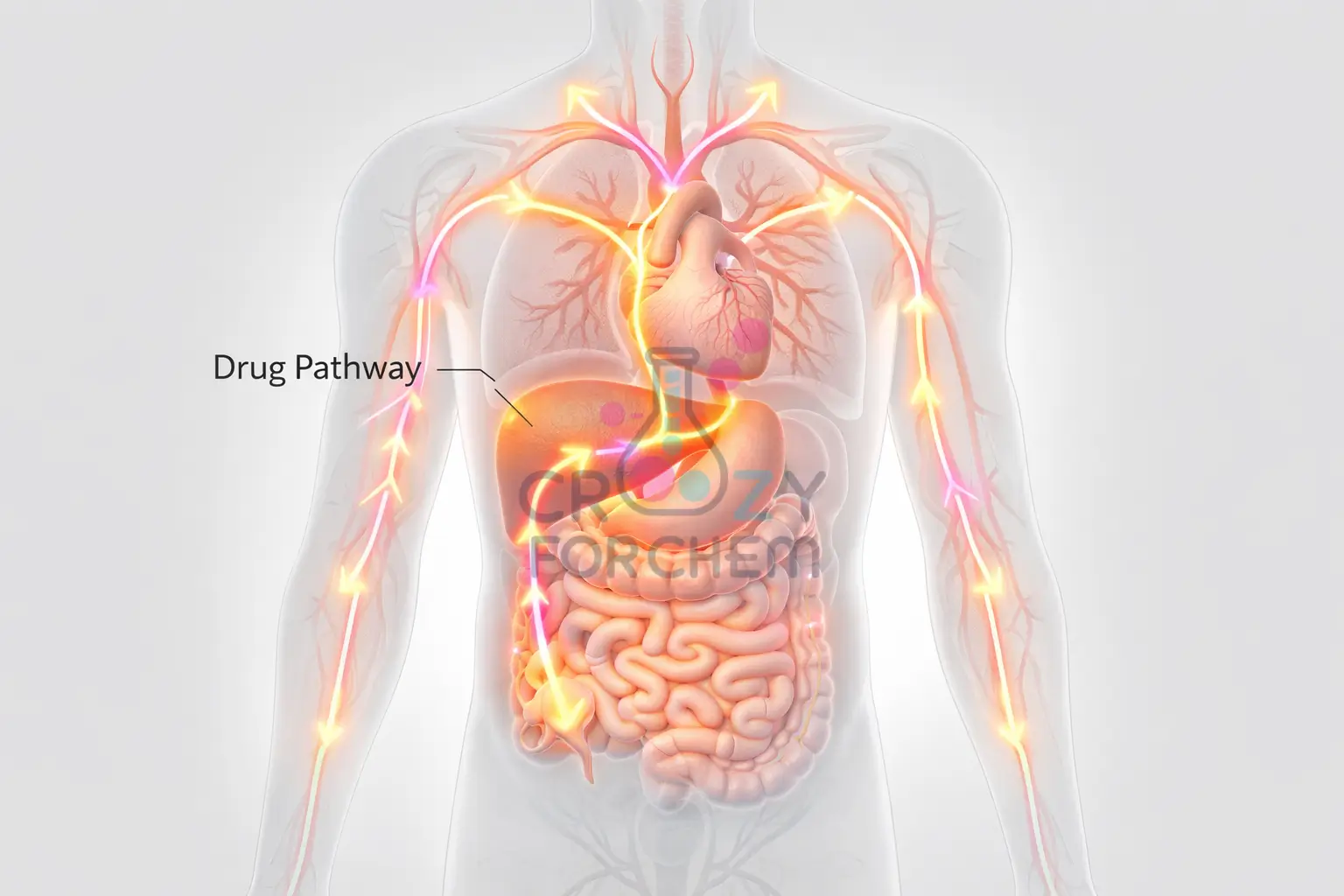
When you swallow a tablet, the active ingredients are absorbed into your bloodstream and pumped by the heart to every tissue and organ in the body.
Local vs. Systemic Action
Only two primary types of painkillers, anti-inflammatories and certain analgesics, can be said to “know” where the site of pain is.
They do this not by searching for the wound, but by reacting to the cytokines and prostaglandins that the body naturally releases at the injury site.
The other types, such as central analgesics and opioids, do not specifically target the wound; they work by reducing the number and strength of pain signals produced by the body or by changing how the brain processes those signals.
The perception is that the pain is reduced at the site because the entire pain transmission system has been “turned down” or suppressed.
The Chemistry of Relief: Aspirin vs. Paracetamol Mechanism
Pain-relief medicines, or analgesics, are broadly categorised by their chemical structure and their specific mechanisms of action.
The Aspirin vs Paracetamol mechanism offers a perfect illustration of how different chemical strategies can achieve similar results.
1. NSAIDs and the Prostaglandin Inhibition Pathway
Non-steroidal anti-inflammatory drugs (NSAIDs), such as Aspirin (ASA), ibuprofen, and naproxen, are brilliant at reducing pain, inflammation, and fever. Their primary goal is prostaglandin inhibition.
They achieve this by inhibiting cyclo-oxygenase (COX) enzymes. By blocking these enzymes, they prevent the production of the prostaglandins that cause pain and swelling.
- Aspirin’s Unique Action: Unlike most other NSAIDs, Aspirin produces a unique, irreversible inactivation of COX enzymes. It achieves this by covalently modifying the enzyme, “locking” it so it can no longer produce inflammatory chemicals.
- The COX-1 vs. COX-2 Distinction: This is a critical technical detail in the Chemistry of painkillers.
- COX-1 is a “constitutive” enzyme found in normal conditions throughout the body; its job is to produce prostaglandins that protect the stomach lining and support kidney function.
- COX-2 is an “inducible” enzyme that appears primarily during inflammatory conditions to trigger pain and fever.
- Traditional NSAIDs block both. Because they inhibit the protective COX-1, long-term use can lead to gastric ulcers, stomach bleeding, and renal damage.
2. Paracetamol: The Central Mystery
Paracetamol (also known as acetaminophen) is used to treat mild-to-moderate pain and fever, but it is not classified as an NSAID because it lacks significant anti-inflammatory properties.
Remarkably, after 150 years of use, the Aspirin vs Paracetamol mechanism for this drug remains somewhat unclear.
It is believed to act primarily centrally, meaning its effects are largely within the brain and spinal cord rather than at the site of injury.
Blocking COX enzymes within the central nervous system raises the body’s overall pain threshold. Because it does not significantly inhibit COX-1 in the stomach, it is generally safer for those with gastric issues than NSAIDs.
3. Potent Interventions: The Science of Opioids
For more intense or severe pain, such as after a surgical procedure or serious trauma, doctors may prescribe opioids (sometimes called narcotics). These substances, which include morphine, codeine, and fentanyl, derive from or mimic natural compounds found in the opium poppy.
The “Earthquake” of Central Suppression
While NSAIDs act like a “molecular crowbar” at the site of injury, opioids work by binding to specific opioid receptors (mu, kappa, and delta) located in the brain and spinal cord.
Blunting the Response: Opioids not only block the signal but also alter the emotional response to pain—patients often report that they can still “feel” the pain, but they no longer “care” about it.
Mechanism of Action: When opioids bind to these receptors, they reduce the excitability of neurons. Pre-synaptically, they close calcium channels to limit neurotransmitter release. Post-synaptically, they open potassium channels, leading to hyperpolarisation. This makes the neuron less likely to transmit a pain impulse.
The Journey of a Tablet: Absorption and Bioavailability
The path a medicine takes from the bathroom cabinet to your cells is a remarkable feat of biochemistry.
1. Swallowing and Dissolution
A common way for painkillers to enter our bodies is via swallowing or chewing. Once in the stomach, all medicines must be dissolved before they can be absorbed into the bloodstream across the membranes of the stomach and small intestine.
2. The Concept of Bioavailability
In the Chemistry of painkillers, a vital concept is bioavailability. This refers to the proportion of the drug that successfully reaches the systemic circulation to produce its effect. Factors such as stomach acidity and the presence of food can affect how much of the drug actually enters the blood.
3. The Liver and First-Pass Metabolism
Blood travels from the stomach to the liver, which acts as a primary filter to remove harmful substances.
Drugs like Aspirin are designed to bind to proteins in the blood, allowing them to pass through the liver undetected initially, so they are not disposed of immediately.
This allows the heart to pump the active medicine to the rest of the body. Eventually, the liver removes the drug from the bloodstream into the bile, and it is excreted from the body five to six hours later.
Specialised Relief: Adjuvant Analgesics
Not all pain responds to traditional NSAIDs or opioids. Neuropathic pain caused by damage to the nerves themselves often feels like burning, tingling, or electric shocks and can be much harder to treat.
- Anticonvulsants: Originally developed for seizures, drugs like gabapentin and pregabalin are first-line treatments for nerve pain. They work by calming overactive nerve cells and affecting calcium channels to reduce abnormal firing.
- Antidepressants: Certain antidepressants, such as amitriptyline and duloxetine, are effective for chronic pain. They work by increasing levels of neurotransmitters like serotonin and norepinephrine in the spinal cord, which help modulate and dampen pain signals.
Side Effects and the Responsibility of Safety
Because these chemicals circulate throughout the entire body, they can affect organs that are not in pain, leading to unintended consequences.
- The NSAID Risk: As mentioned, the COX-1 vs COX-2 distinction explains why NSAIDs can cause gastric damage, kidney problems, and increased bleeding tendencies.
- The Paracetamol Ceiling: While safe at recommended doses, paracetamol is the most frequently overdosed medicine. Because it is metabolised by the liver, an overdose can cause permanent, life-threatening liver failure.
- Opioid Tolerance and Addiction: Regular use of opioids can lead to tolerance, where a person needs higher and more frequent doses to achieve the same relief. Because they activate reward centres in the brain and produce euphoria, they carry a high risk of physical dependence and addiction, known as opioid use disorder (OUD).
Conclusion: Empowerment Through Knowledge
Understanding the Chemistry of painkillers transforms a routine trip to the medicine cabinet into an informed scientific decision.
These medications are a true marvel of modern medicine, capable of bringing immense comfort and enabling recovery from serious injury. However, their power demands respect.
By understanding how painkillers work and being aware of the Aspirin vs Paracetamol mechanism, you can choose the right tool for your specific type of pain.
Whether it is managing the risks of prostaglandin inhibition or recognising the dangers of opioid dependency, knowledge is your best defence.
Always use the lowest effective dose for the shortest time possible, and never hesitate to seek professional medical advice for persistent or severe pain.
Frequently Asked Questions
-
How does a painkiller know where the pain is located?
Painkillers do not actually “know” the location of your injury. After ingestion, the active ingredients circulate through your entire bloodstream. NSAIDs (like Aspirin) work by blocking COX enzymes throughout the body, which stops the production of prostaglandins (pain signals). You only perceive the relief at the injury site because that is where the highest concentration of these distress signals was being produced.
-
Why don’t painkillers make my whole body feel numb?
Analgesics only target specific chemical pathways, not all sensory nerves. Unlike a local anaesthetic that blocks all sensation (including touch and temperature), over-the-counter painkillers only inhibit the specific enzymes or receptors involved in the pain and inflammation pathway. Your touch receptors remain fully functional.
-
Why does Aspirin work faster than some other tablets?
The speed of relief depends on the drug’s Bioavailability and dissolution rate. Dispersible or effervescent Aspirin dissolves rapidly in the stomach’s acidic environment, allowing the active molecules to enter the bloodstream more quickly. In contrast, enteric-coated tablets are designed to bypass the stomach and dissolve in the small intestine, which delays the onset of action.
-
How long do painkillers take to start working?
Most oral analgesics begin to take effect within 20 to 30 minutes. This is the time required for the tablet to dissolve, pass through the stomach lining, and undergo first-pass metabolism in the liver before reaching a therapeutic concentration in your systemic circulation.
-
Is it safe to take painkillers with antibiotics?
Generally, yes, as they operate on entirely different biological systems. Antibiotics target bacterial cell walls or protein synthesis, while painkillers target human enzymes or nervous system receptors. However, if an antibiotic causes stomach irritation, it is best to avoid NSAIDs like Ibuprofen or Aspirin, as they can further irritate the gastric lining. Always consult a pharmacist for specific drug-drug interactions.
-
Why can’t I take more than the recommended dose of Paracetamol?
Paracetamol has a strict “Ceiling Effect” and a high risk of hepatotoxicity. Once your liver’s metabolic pathways are saturated, the drug is broken down into a toxic by-product called NAPQI. An overdose can lead to irreversible liver failure because the body runs out of glutathione to neutralise this toxin.
-
Can I use bleach-based cleaners while taking these medicines?
Yes, but ensure proper ventilation. As discussed in [Cluster 8], mixing bleach with ammonia creates toxic gases. While there is no direct chemical interaction with swallowed pills, the respiratory distress from chloramine gas can exacerbate the symptoms of any underlying condition you are treating.